WHAT IS CONNECTIVITY?
Connectivity is the name of the Waterloo Region “Situation Tables”, which bring police, health and social service agencies together at a weekly meeting to collaboratively and proactively address situations of acutely elevated risk in the community.
In January 2014, the Waterloo Regional Police Service (WRPS) in partnership with Langs Community Health Centre implemented a Situation Table in Cambridge. In partnership with Carizon Family and Community Services, a second Situation Table became operational in Kitchener in October 2014.
Connectivity is about building stronger connections across workers in the local justice, health and social service sectors in order to connect community members in situations of acutely elevated risk to the help they need more quickly.
EVALUATING CONNECTIVITY
In January 2015, Langs, Carizion, and WRPS partnered with Taylor Newberry Consulting to
carry out a first phase of evaluation of the Connectivity Tables. You can read more about the Connectivity model and our past evaluation findings here, as well as download the full report and summary.
Phase 1 of the evaluation that examined the operations and collaborative practices of Connectivity. Following this, the leadership requested a Phase 2 evaluation that was more heavily focused on outcomes. Taylor Newberry Consulting continued this evaluation work in 2016-2017.
We encourage you to read the full Phase 2 report for more detail!
An Executive Summary is also available.
KEY EVALUATION QUESTIONS GUIDING PHASE 2
- To what extent do individuals engage with the supports and services developed and implemented by Connectivity?
- What new services and supports do individuals access to meet their needs?
- What are individuals’ experiences with new supports and services? Are they experienced as beneficial and helpful? In what ways? How can services be improved?
- What changes are observed in people’s lives? To what extent are stability and wellness promoted? How is risk mitigated or removed?
- To what extent have interventions by Connectivity influenced the frequency and duration of emergency department visits and hospital admissions among Connectivity users?
- To what extent have interventions by Connectivity influenced the frequency of police service calls among Connectivity users?
HIGHLIGHTS OF THE PHASE 2 EVALUATION FINDINGS
- Ongoing success of the tables relies on assembling multi-disciplinary teams that have a strong outreach capacity to access individuals in the community, as well as a tenacious, “whatever it takes” commitment to addressing needs. Table members need support and endorsement from their parent organizations to overcome recurring service barriers.
- Strategic collaboration of particular organizations and resources appeared to be effective in a number of situations – the coordinated intervention of police, housing services, community mental health services, and hospital intervention. Specifically, the ability of Connectivity to work proactively with hospitals to ensure admission and the mobilization of community supports and, often, psychiatry, was important.
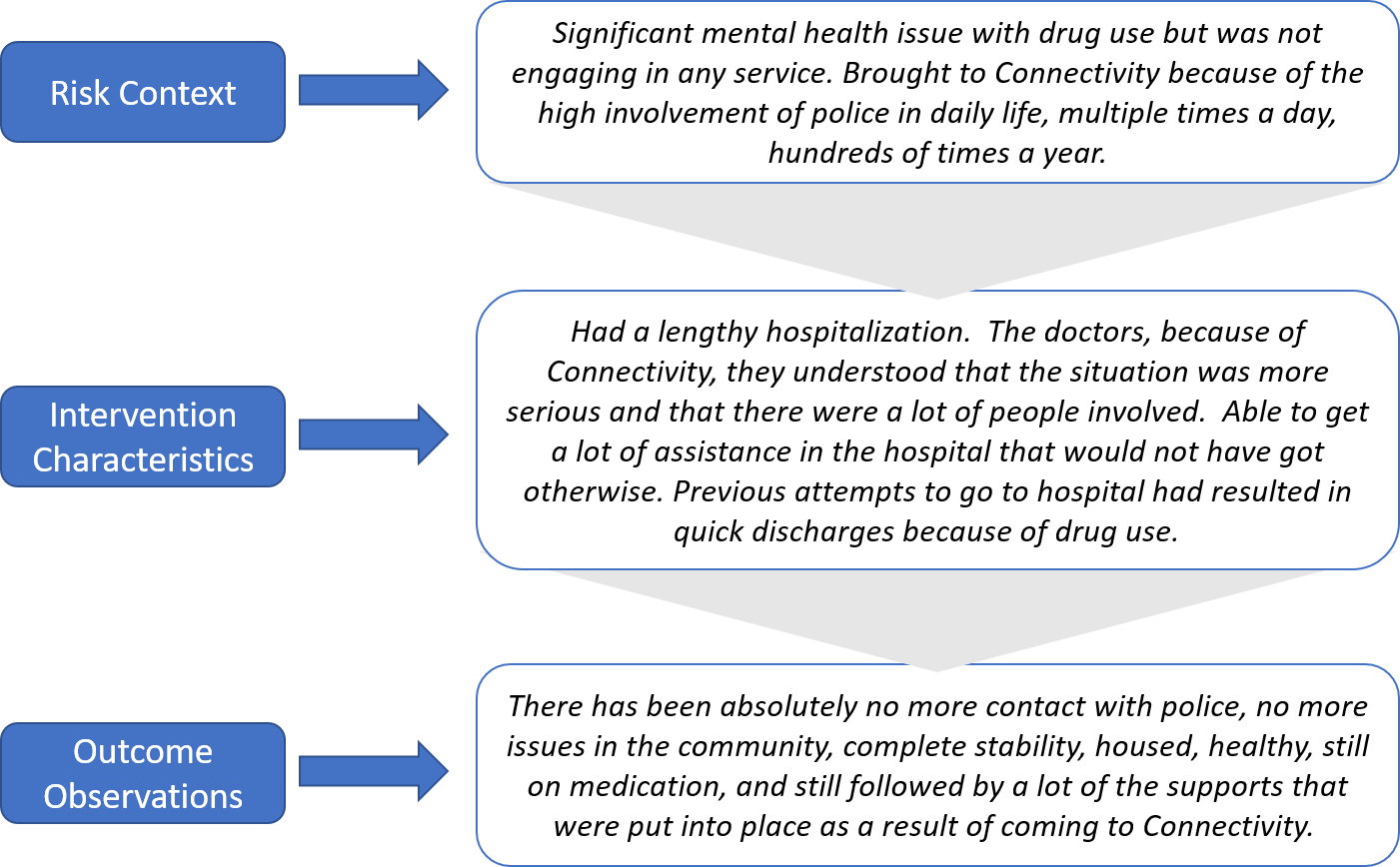
- Qualitative interviews provided numerous examples of success, where individuals moved from serious risk contexts to ongoing service connections, stability and functioning, and improvements in quality of life. Below is an example of risk context, intervention characteristics, and outcome observations (note: these are quotes are slightly paraphrased from our interviews to remove identifying information, including personal pronouns).
- The general success of Connectivity is qualified by ongoing challenges in engaging individuals presenting with drug addictions. Table members identified use of crystal methamphetamine as particularly challenging risk factor. About 50% of individuals whose situations were closed as “Connected” had drug use as a risk factor; in comparison about 80% of individuals whose situations were closed as “Still At-Risk”, had drug use as a risk factor.
- A range of service and system barriers continue to persist in Waterloo Region, hampering the efforts of Connectivity in mitigating risk and fostering longer-term positive outcomes. These include early discharge from hospital (especially when addictions are presenting), poor access to detox services and long wait lists for addictions treatment, a lack of discharge planning out of prison, lengthy wait lists for longer term supports and services (e.g., mental health support coordination, addictions treatment), and a lack of affordable housing options.
- Analysis of data provided by Cambridge Memorial Hospital (CMH) and Grand River Hospital (GRH) showed 14% and 69% decreases, respectively, in emergency department visits after Connectivity interventions. Length of stay increased 31% at CMH and decreased 44% at GRH (however, the absolute number of in-patient days was quite small at GRH both before and after Connectivity intervention, which strongly qualifies the percent decrease). The drop in ED visits represents $40 thousand of diverted costs.
- Analysis of data provided by Waterloo Regional Police Services (WRPS) shows 46% decrease in repeat police calls between 90-day periods, before and after Connectivity. Conservatively estimated, this represents just under $100 thousand available for other allocations.